

Analgesics in the ED: What Works, What Doesn’t
/

Tired of reading? Prefer to absorb your MedEd through your wonderful powers of hearing? Check out our podcast HERE
Prompt, safe, and effective pain management is a core competency of the emergency provider. Unfortunately, traditional strategies for administering analgesics for acute pain have shown poor success rates. In this podcast episode, Dr. Matthew Delaney shares a few evidence based pain management pearls you can use on your next shift.
THE TRADITIONAL APPROACH TO ADMINISTERING IV MORPHINE AND HYDROMORPHONE WORKS POORLY
The “text book” doses of morphine and hydromorphone underperform for pain control when given as a single dose. [1]


PROTOCOLS FOR THE TIMING AND DOSING OF IV MORPHINE AND HYDROMORPHONE CAN INCREASE YOUR SUCCESS
Current re-dosing protocols for IV analgesics can be logistically challenging.[2]
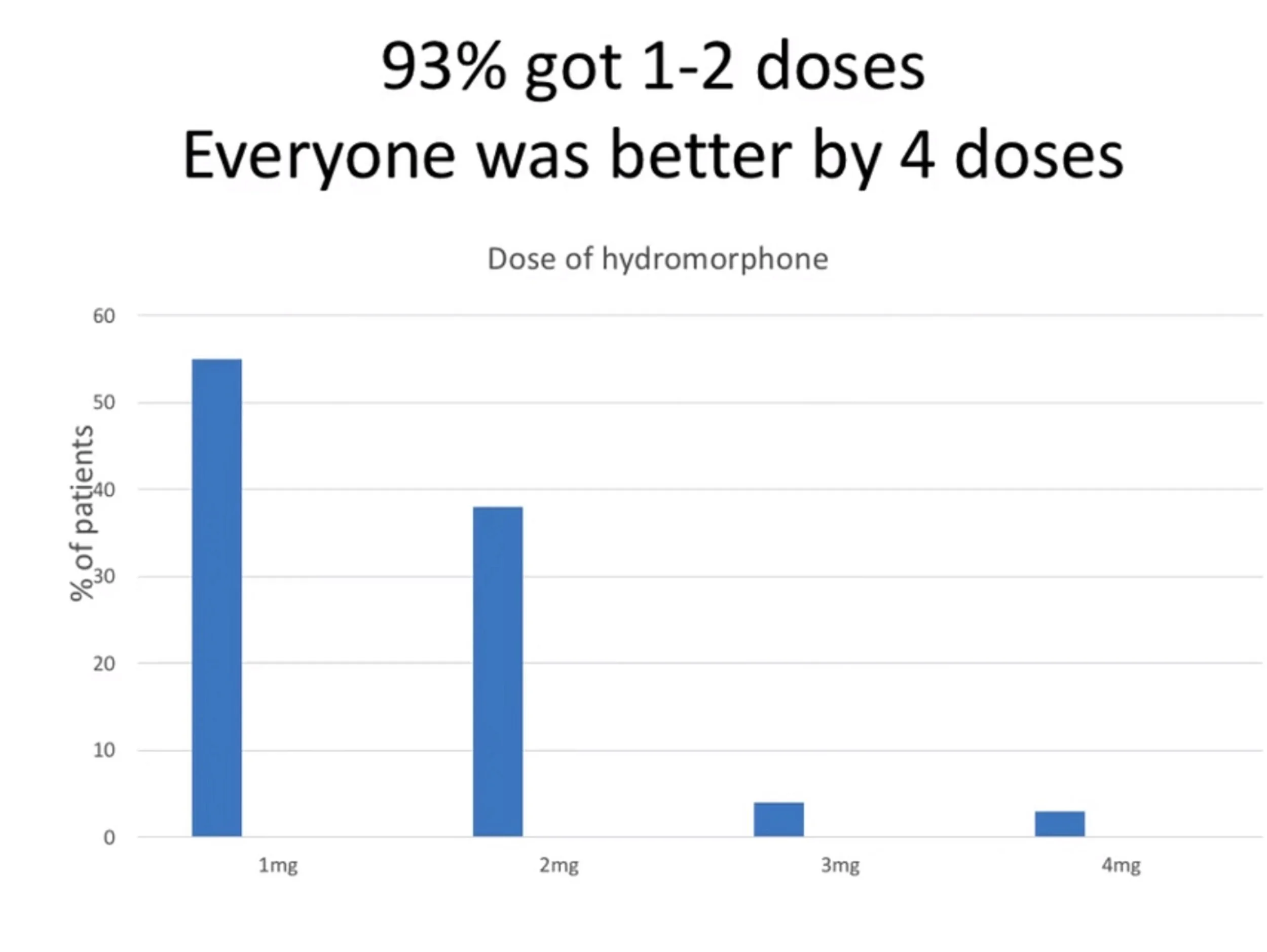
One simple protocol by Chang et al. asked the patient every 30 minutes if they needed additional doses of IV hydromorphone (up to 3 doses). This protocol provided adequate analgesia in 99% of cases.[3]
CHANG eT AL.
ORAL OVER THE COUNTER COMBINATIONS OUTPERFORM MOST OTHER ANALGESICS
Combinations of acetaminophen and ibuprofen at varying doses provide superior pain relief to most commonly prescribed oral analgesics.[4,5]
NUMBER NEEDED TO TREAT FOR >/= 50% REDUCTION IN PAIN

mOORE ET AL
CONSIDER TOPICAL NSAIDS FOR PAIN CONTROL
Topical NSAIDs combine the analgesic properties of oral NSAIDs with the placebo effect from the use of a lotion.
This may be a good option for patients who report intolerance (or may be at higher risk of adverse effects) to oral NSAIDs.
Patients experienced moderate rates of skin irritation but have essentially no GI or systemic adverse effects. [6,7]
TOPICAL NSAIDs - NUMBER NEEDED TO TREAT
FOR >/= 50% REDUCTION IN PAIN

The only topical NSAID available in the US is diclofenac sodium gel (Voltaren).
A reasonable dosing strategy is to instruct the patient to apply an almond size amount of gel to the affected
area 3 x daily.

CLICK HERE TO CHECK OUT OUR PODCAST

.
Edited and Posted by Jeffrey A. Holmes, MD
Original content and authorship by Matthew Delaney, MD
Dr. Delaney has no disclosures or conflicts of interest.
References
1. Bijur PE, Kenny MK, Gallagher EJ. Intravenous morphine at 0.1 mg/kg is not effective for controlling severe acute pain in the majority of patients. Ann Emerg Med. 2005 Oct;46(4):362-7. PubMed PMID: 16187470. [Pubmed]
2. Lvovschi V, Aubrun F, Bonnet P, Bouchara A, Bendahou M, Humbert B, Hausfater P, Riou B. Intravenous morphine titration to treat severe pain in the ED. Am J Emerg Med. 2008 Jul;26(6):676-82. doi: 10.1016/j.ajem.2007.10.025. PubMed PMID: 18606320.[Pubmed]
3. Chang AK, Bijur PE, Holden L, Gallagher EJ. Efficacy of an Acute Pain Titration Protocol Driven by Patient Response to a Simple Query: Do You Want More Pain Medication? Ann Emerg Med. 2016 May;67(5):565-72. doi: 10.1016/j.annemergmed.2015.04.035. Epub 2015 Jun 11. PubMed PMID: 26074387.[Pubmed]
4. Moore RA, Derry S, Aldington D, Wiffen PJ. Single dose oral analgesics for acute postoperative pain in adults - an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015 Sep 28;(9):CD008659. doi: 10.1002/14651858.CD008659.pub3. Review. PubMed PMID: 26414123.[Pubmed]
5. Moore RA, Wiffen PJ, Derry S, Maguire T, Roy YM, Tyrrell L. Non-prescription (OTC) oral analgesics for acute pain - an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015 Nov 4;(11):CD010794. doi:10.1002/14651858.CD010794.pub2. Review. PubMed PMID: 26544675.[Pubmed]
6. Tugwell PS, Wells GA, Shainhouse JZ. Equivalence study of a topical diclofenac solution (pennsaid) compared with oral diclofenac in symptomatic treatment of osteoarthritis of the knee: a randomized controlled trial. J Rheumatol. 2004
Oct;31(10):2002-12. PubMed PMID: 15468367.[Pubmed]
7. Klinge SA, Sawyer GA. Effectiveness and safety of topical versus oral nonsteroidal anti-inflammatory drugs: a comprehensive review. Phys Sportsmed. 2013 May;41(2):64-74. doi: 10.3810/psm.2013.05.2016. Review. PubMed PMID:
23703519.[Pubmed]








