

Acute Otitis Media- do you really know what you're doing?
/
The Podcast
Tired of reading? Prefer to absorb your MedEd through your wonderful powers of hearing? Check out our conversation with Dr. Daria Thompson, a pediatric hospitalist, on this very topic! Click here.

In this blog post we talk ear infections, or Acute Otitis Media (AOM) - a common disease commonly diagnosed... and probably commonly done wrong. We'll talk definitions of disease, common alternative diagnoses, and treatment plans by age. I assure you- you'll learn something new.
To open, let’s consider some scenarios:

Scenario 1: A 22 month old girl comes in with fever and acting irritable. Mom says there has been no real cough, but a little runny nose all winter long. Her fever was to 38.8 C this morning, then tactile this afternoon and controlled with Tylenol. She looks well, with normal vital signs but Tylenol was given only two hours ago. Her right ear is erythematous, bulging and has an effusion.

Scenario 2: A 4 year old boy comes in complaining of ear pain. Mom notes he has been complaining of an earache since last night so they came in to be evaluated. He is well appearing without a fever. The left tympanic membrane (TM) has the appearance of some opacification, maybe some scarring, and an effusion.
Scenario 3: An 11 year old girl comes in with a cough, runny nose, ear pain and a fever to 38.5 C earlier today. Physical exam shows lots of rhinorrhea, dry cough, and normal lung auscultation. Both ears are erythematous, left greater than right, and her left TM has an effusion.


Defining Acute Otitis Media

American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. (Reference 2)
The definition of AOM is important to outline as there are several similar diseases or look-alikes that can confuse the clinician, such as Otitis Media with Effusion (OME), which is generally NOT an acute infectious process (it is often the sequelae of a recent viral URI or related to eustachian tube dysfunction).
Treatment Algorithm by Age
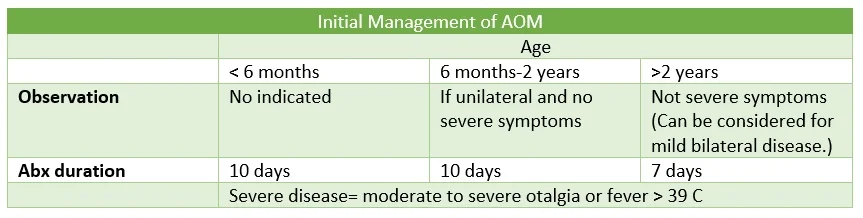
Once AOM is diagnosed, we next have to make a decision about treatment. In particular, we must ask ourselves “does this patient need antibiotics?” The answer is not universally YES. The notion of “watchful waiting” is well supported in AOM and is an opportunity to practice good antibiotic stewardship in Emergency Medicine.
So who needs antibiotics? Well, to answer that we need to assess 1) patient age and 2) severity of symptoms.
Clinical Pathway for Evaluation/Treatment of Acute Otitis Media in Children 2 Months to 12 Years Old (REference 3)
Severe disease is typically defined as a fever > 39 C, which is easy to identify, or moderate to severe otalgia… a much more nebulous term for little ones. One easy way to quantify this pain is by its effect on activities of daily living (ADLs). If a little tylenol or ibuprofen brings the patient back to their happy and playful self, then it is not severe. If they are still noting pain, are excessively fussy, disinterested in eating/drinking or normal play, consider it severe disease.
Observation or “watchful waiting” is only trialed for 48-72 hours. If symptoms progress or fail to improve during that time frame, antibiotic therapy should be instituted.
**It is worth noting that slight differences exist between the 2004 recommendations from the American Academy of Pediatrics/American Academy of Family Physicians joint paper [PDF] (treat all six month to two year old children with diagnostic certainty for AOM) and the 2013 American Academy of Pediatrics practice guideline paper [PDF] (includes watchful waiting).
Antibiotic Selection

Clinical Pathway for Evaluation/Treatment of Acute Otitis Media in Children 2 Months to 12 Years Old (Reference 3)
So you decided to treat a patient for AOM - either they are less than six months old, have severe symptoms, or failed a trial of watchful waiting. Which antibiotic should you use?
The backbone of most treatment for AOM is good ol’ amoxicillin. Other options are patient specific and outlined in the table “antibiotic therapy options for AOM.”
Scenario Wrap Up
Scenario 1: A 22 month old girl comes in with fever and acting irritable. Mom says there has been no real cough, but a little runny nose all winter long. Her fever was to 38.8 C this morning, then tactile this afternoon and controlled with Tylenol. She looks well, with normal vital signs but Tylenol was given only two hours ago. Her right ear is erythematous, bulging and has an effusion.
This young girl has a clear cut AOM, but is in the age range for watchful waiting and does not meet any of the severe disease criteria. A consideration for a 48-72 hour watchful waiting approach can be considered in discussion with the patient’s caregiver.
Scenario 2: A four year old boy comes in complaining of ear pain. Mom notes he has been complaining of an earache since last night so they came in to be evaluated. He is well appearing without a fever. The left tympanic membrane (TM) has the appearance of some opacification, maybe some scarring, and an effusion.
This child has otitis media with effusion and not acute otitis media. This disease process generally does not require antibiotics.
Scenario 3: An 11 year old girl comes in with a cough, runny nose, ear pain and a fever to 38.5 C earlier today. Physical exam shows lots of rhinorrhea, dry cough, and normal lung auscultation. Both ears are erythematous, left greater than right, and her left TM has an effusion.
This is a tougher one. The patient is older and has URI symptoms which could have caused her left ear effusion. She could also have a concurrent left AOM on top of her URI. That said, she is certainly in an age range where watchful waiting could be used and she does not have features of severe disease. Watchful waiting is recommended.
Here is the audio of my interview with Dr. Daria Thompson:
Another lecture on AOM
If you want to learn even MORE on AOM, check out Dr. Nathan Mick’s lecture.
References
Lieberthal AS, Carroll AE, Chonmaitree T, Ganiats TG, Hoberman A, Jackson MA, Joffe MD, Miller DT, Rosenfeld RM, Sevilla XD, Schwartz RH, Thomas PA, Tunkel DE. The diagnosis and management of acute otitis media. Pediatrics. 2013 Mar;131(3):e964-99. [PDF]
American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004 May;113(5):1451-65. [PDF]
Children's Hospital of Philadelphia (CHOP) AOM diagnosis and therapeutic algorithm [website]
American Family Physician: Otitis Media- Diagnosis and Treatment [website]
American Family Physician- Should Children with Acute Otitis Media Routinely Be Treated with Antibiotics? No: Most Children Older Than Two Years Do Not Require Antibiotics. [website]







