

Sim Cliff Notes - June 2017
/
Every month we summarize our simulation cases. No deep dive here, just the top 5 takeaways from each case. This month's cases included death notification, elder abuse, refusal of medical care (AMA).
Five step process to Death Notification

http://www.istockphoto.com/photos/doctor-bad-news-couple-sadness?excludenudity=true&sort=mostpopular&mediatype=photography&phrase=doctor%20bad%20news%20couple%20sadness
1. Prepare to give the news
- See the family as soon as possible.
- Set time aside to talk to the family, silence your phone/pager.
- Ensure that you are presentable.
- Take a moment to address your emotions if necessary.

2. The introduction
- Introduce yourself and your role.
- Confirm to whom you are speaking.
- Find out what the family knows - this will help set the stage for the amount of information that needs to be communicated before the actual death notification.
- Fire the 'warning shot across the bow' early in the converations ("I am afraid I have some bad news")
- It is appropriate to set the tone early

3. The notification
- Share information with a pace and wording (no medical jargon) they can handle.
- Use concrete language such as "he died"... no euphemisms such as "he has passed" or "he is in a better place."
4. Allow the grieving process
- Allow people to express grief in their own way.
- Avoid comments such as “it was God’s will”
- Express sympathetic comments
- Ask the family if they would like to see the patient (never the "body")
- Ask if the family would like to see a pastor
- Regardless of the family's denomination, pastors are very skilled grief counselors
- Provide contact information if you are comfortable so family can call later with any additional question
- I offer them my department's administrative assistant's phone number
- It is unlikely the family will remember much of your conversation after the death notification and it is helpful to give them a contact for any future questions
5. Don't forget to take care of yourself
- Take a brief moment before you go back to work.
- A future debrief with friend/colleague can be extremely helpful.
- Reach out to hospital services for support if needed.
References
1. Tolle SW, Girard DE. The physician’s role in the events surrounding patient death. Arch Intern Med 1983;143:1447-1449.
2. Olsen JC, Buenefe ML, Falco WD. Death in the emergency department. Ann Emerg Med 1998;31:758-765.
3. Buckman R. Breaking bad news: Why is it so difficult? BMJ 1984;288: 1597-1599.
4. Iserson KV. The gravest words: Sudden-death notifications and emergency care. Ann Emerg Med 2000;36:75-77.
5. Swisher LA, Nieman LZ, Nilsen GJ, et al. Death notification in the emergency
department: A survey of residents and attending physicians. Ann Emerg Med 1993;22:1319-1323. 6.Viswanathan R, Clark JJ,Viswanathan K. Physicians’ and the public’s attitudes on communication about death. Arch Intern Med 1986;146:2029-2033.
7. Parrish GA, Holden KS, Skiendzielewski JJ, et al. Emergency department experience with sudden death: A survey of survivors. Ann Emerg Med 1987;16:792-796.
8. Jurkovich GJ, Pierce B, Pananen L, et al. Giving bad news: The family perspective. J Trauma 2000;48:865-870.
9. Adamowski K, Dickinson G,Weitzman B, et al. Sudden unexpected death in the emergency department: Caring for the survivors. Canadian Medical Association Journal 1993;149:1445-1451.
10. Jones WH. Emergency room sudden death: What can be done for the survivors? Death Education 1978;2:231-245.
Elder abuse
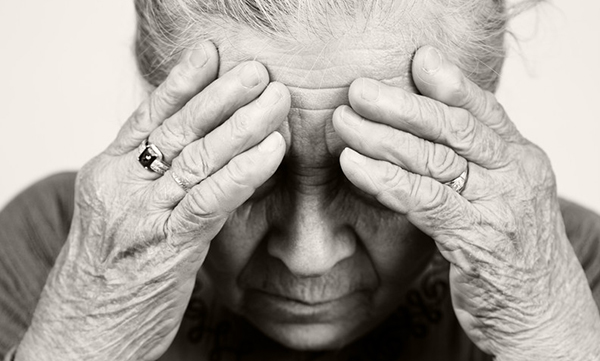
http://reachofhaywood.org/elder-abuse/
1. If you don't think about it and screen for it, you could miss a rare chance to help a victim.
- Elder abuse is generally defined as physical, sexual and emotional abuse, financial exploitation, neglect and self-neglect, and abandonment of an older person (NCEA, 2004).
- The abuser (a family member in 90% of cases) feels a sense of entitlement to use various forms of abuse to gain and maintain power and control over the victim.
- Abusers will use a pattern of coercive tactics and whatever method necessary, including isolation, intimidation and threats, withholding food, medication and sleep, and physical and sexual abuse to get their way (Schechter, 1987).
2. Listen and look for red flags that indicate elder abuse.
- From a victim:
- Appears isolated
- Says or hints at being afraid
- Considers or attempts suicide
- Has history of substance abuse (including prescription drug abuse)
- Presents as a "difficult" patient
- Has vague, nonspecific complaints
- Is unable to follow through on treatment plans or medical care; they may miss appointments
- Delays seeking medical care
- From a potential abuser:
- Is verbally abusive to staff in public or is charming and friendly to service providers
- Says things like “he’s difficult,” “she’s stubborn,” “he’s so stupid,” or “she’s clumsy”
- Attempts to convince others that the person is incompetent, stupid, or crazy
- Is “overly attentive” to the person
- Controls the person’s activities
- Refuses to allow interview or exam to take place without being present (often answers for the victim)
- Talks about the person as if he or she is not a person
3. First do no harm - you want to help a victim of elder abuse, not alienate them.
- DO everything possible to give a victim a sense of hope by:
- Believeing the account of the abuse
- Sharing that abuse can happen to anyone and the victim is not alone
- Affirming that the victim is not to blame for the abuse
- Planning for safety or finding someone who can
- Offering options and giving information about resources or finding someone who can
- Keeping information shared by the victim confidential
- Documenting the abuse with photographs, body maps and victim statements
- DO NOT do anything that further isolates, blames, or discourages victims, such as:
- Telling the victim what to do (e.g., “you should leave immediately”)
- Judging a victim who returns to an abusive relationship
- Threatening to or ending services if a victim does not do what you want
- Breaking confidentiality by sharing information with the abuser or other family members
- Blaming the victim for the abuse (“if only you had tried harder or done this, the abuse might not have happened")
- Reporting abuse to the authorities without permission from the victim (unless mandated by law - Maine has mandatory reporting). If you are a mandated reporter, tell the victim what you are doing and why. Help the victim with safety planning or find someone who can.
4. DO NOT collude with the abuser and give him/her more power and control by:
- Accepting excuses from the abuser and supporting the violence (“I can understand how much pressure you are under. These things happen.”)
- Blaming drugs/alcohol, stress, anger, or mental illness for the abuse. Abusers must be held accountable for their actions before they will change their behavior.
- Minimizing the potential danger to the victim or yourself if you offer help.
- Arrange for appropriate security for the victim and your staff when working with a potentially lethal batterer (e.g., has made homicidal/suicidal threats or plans, owns weapons, is fixated on victim).
5. Work collaboratively to help your victim.
- To learn more about potential interventions, contact local domestic abuse and/or sexual assault, victim/witness, or adult protective services/elder abuse agencies.
- With the victim’s permission, refer to appropriate agencies for assistance.
- Use experts in a variety of fields as case consultants on difficult cases. Bring challenging cases to a multidisciplinary teams for review. Ensure client confidentiality.
Adapted from the National Clearing House on Elder Abuse - "Tips on working with older Victims"
References
1. Brandl, B. (2002). From a Web of Fear and Isolation to a Community Safety Net. Madison, Wisconsin, 53703-3041. National Clearinghouse on Abuse in Later Life.
2. Schechter, S. (1987). Guidelines for Mental Health Workers. Denver, Colorado. National Coalition Against Domestic Violence.
3. National clearing house on elder abuse (www.ncall.us)
4. Rosen T, Hargarten S, Flomenbaum NE, Platts-Mills TF. Identifying elder abuse in the emergency department: Toward a multidisciplinary team-based approach. Ann Emerg Med. 2016. http://www.ncbi.nlm.nih.gov/pubmed/27005448
5. Lachs MS, Pillemer KA. Elder abuse. N Engl J Med. 2015;373(20):1947-1956. http://www.ncbi.nlm.nih.gov/pubmed/26559573
6. Dong XQ. Elder abuse: Systematic review and implications for practice. J Am Geriatr Soc. 2015;63(6):1214-1238. http://www.ncbi.nlm.nih.gov/pubmed/26096395
7. Gibbs LM. Understanding the medical markers of elder abuse and neglect: Physical examination findings. Clin Geriatr Med. 2014;30(4):687-712. http://www.ncbi.nlm.nih.gov/pubmed/25439636
Refusal of Medical Care ("Leaving Against Medical Advice")

https://pixabay.com/en/photos/exit%20sign/
1. Don't take it personally.
- This clinical scenario is particularly difficult as it pits our duty to help our patients against our duty to respect their autonomy.
- The patient who wishes to refuse medical care often appears as though they "know better" and don't respect your opinion as a provider. Try not to let your ego get in the way. Providing optimal care is all about maximizing your workup/therapy within the given constraints of the patient.
2. Communicate, negotiate and involve others.

- The majority of AMA cases are a failure of communication, not of capacity. I think a large number of AMA cases can be avoided by making sure we understand our patient and they understand us.
- Attempt to identify and resolve the reason for refusal of medical care.
- Is their PTSD from their three tours in Iraq making them anxious and wanting to leave?
- Is your patient afraid of another medical bill that they can't afford?
- Does your patient have three cats at home they have to feed? (I swear this is all too common!)
- There is usually room for negotiation with your patients
- A meal tray or nicotine patch can sometimes go a long way.
- Involving others (a patient's family, spouse, primary care physician, specialist) can help facilitate negotiation.
- If the patient refuses admission, ask if you can arrange for continued outpatient workup/treatment and follow up.
- E.g. if a sick patient with pneumonia refuses admission then the next best option can be offered (IV fluids, outpatient antibiotics, close follow up with PCP).
3. Assess the patient's capacity to refuse medical care.
- Normal findings on the mental status examination without evidence of diminished mental capacity from closed head injury, severe pain, hypoxia, hypotension, alcohol intoxication, mental retardation, or mind-altering substances constitute good evidence of competency.
- Noting the patient’s rationale for refusing care, even if it is not reasonable, provides additional evidence of competency.
4. Ensure informed refusal.
- Give the patient all the relevant information:
- His or her current condition
- Therapeutic options (including the alternative)
- The risks and benefits of these options
- Have the patient explain the reason for their choice
- Have the patient paraphrase the information you have told them to ensure understanding
5. Document well.
- Having a patient sign out "AMA" is a process, not a form.
- Make sure you document the patient's capacity and components of informed refusal.
Written by Jeffrey A Holmes, MD








